AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2693-4779/049
*Corresponding Author: Jochanan E. Naschitz, Bait Balev Nesher and The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
Citation: O Zalyesov, M Badarny, N Zaygraykin, J E. Naschitz. (2021) Use of the frailty tools FI MDS and FI Rockwood to predict outcomes of inpatient rehabilitation after proximal hip fracture. Clinical Research and Clinical Trials. 4(1); DOI: 10.31579/2693-4779/049
Copyright: © 2021 Jochanan E. Naschitz, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 June 2021 | Accepted: 28 June 2021 | Published: 02 July 2021
Keywords: frailty; hip fracture; rehabilitation; functional independence measure (FIM); clinical frailty scale; inpatient rehabilitation; MMSE
Background Among factors which affect the outcome of rehabilitation after hip fracture, the role of pre-fracture frailty has not been defined.
Objective To assess the impact of frailty on rehabilitation outcome in elderly persons with proximal hip fracture. Setting Geriatric rehabilitation center.
Design Retrospective observational study.
Subjects Forty consecutive patients with proximal hip fracture.
Methods The following parameters were calculated: FI-MDS frailty index, Rockwood Clinical Frailty Scale (FI Rockwood), Functional Independence Measure (FIM) on discharge, absolute functional gain (ΔFIM), length of stay (LOS), and FIM gain per day (ΔFIM/LOS). FIM discharge ≥90 and motor FIM discharge >58 indicated success in rehabilitation.
Results There were 31 women and 9 men, mean age 80 years. The mean pre-fracture FI MDS was 10 points (SD 5.8) out of 58 possible, the mean FI Rockwood score was 3 (SD 1.7) out of 7 possible. The mean admission FIM was 76.6 (SD 16), the mean discharge FIM was 92.7 (SD 19.3), mean LOS 22.5 days (SD 9.7), mean ΔFIM/LOS 0.8 (SD 0.6). Pre-fracture frailty was associated with worse outcome of rehabilitation: FI MDS predicted discharge FIM ≥90 with OR 0.86, p 0.012; FI Rockwood predicted discharge FIM ≥90 with OR 0.68, p 0.027; FI MDS predicted discharge motor FIM >58 with OR 0.91, p 0.07; FI Rockwood predicted discharge motor FIM >58 with OR 0.71, p 0.027.
Conclusions Though pre-fracture frailty correlated with FIM on discharge, neither frailty tool was specific enough to predict success in rehabilitation and the necessary length of rehabilitation. Translating frailty scores in tools adequate for clinical decision making remains an aim for future studies.
1. Among factors which shape the outcome of rehabilitation after hip fracture, the role of frailty is not well defined.
2. Two frailty tools were used in the present study: the FI-MDS frailty index and the Rockwood Clinical Frailty Scale.
3. Both are appropriate for subjects with physical and cognitive limitations.
4. Our study showed an inverse correlation between pre-fracture frailty and achievement in rehabilitation.
5. Tough reliable and easy to use, neither FI-MDS nor the Rockwood Clinical Frailty Scale were specific in predicting successful rehabilitation after hip fracture.
Numerous factors affect the outcome of rehabilitation in patients with hip fractures, including the patient's age, gender, pre-fracture functional ability, cognitive condition, affective status, comorbidity, social support, and the number of treatments [1-5]. The outcome of inpatient rehabilitation after hip fracture surgery may well be affected by frailty that pre-existed to hip fracture. It is assumed that frailty tools may help in guiding management decisions in patient care [6-13].
Frailty is understood as the increased vulnerability to stressors and limited homeostatic reserves to stabilize declines across multiple physiologic systems. Adults who are frail are prone to developing disease and have worse disease outcomes. Frailty that predicts greater clinical risk [14]. No single frailty assessment tool has become dominant. Fried LP et al. labeled an operational phenotype of frailty. Accordingly, frailty is a clinical syndrome in which three or more of the following alterations are present: unintentional weight loss (4.5 kg in the past year), self-reported exhaustion, weakness (by grip strength measurement), slow walking speed, and low level of physical activity [15]. Many other frailty scores have been proposed [16-20]. Ideally a frailty tool should be quick, reliable, and easy to use in clinical settings. These demands are not met by most frailty tools which are in common use but are well served by two instruments: the FI-MDS frailty index [21] and the Rockwood Clinical Frailty Scale [22]. The two latter do not require examination of physical performance nor the need of patients’ self-reporting their impairments. The FI MDS and FI Rockwood are informed by cognitive, motor and social functioning, disability and morbidities, influenced by psychological factors and social support. Thus, the frailty score is the equivalent of a battery of tests. The FI MDS and FI Rockwood are both appropriate for use in subjects with physical impairment and cognitive decline, features often met in older subjects recovering from hip fracture.
In the present study we assessed whether pre-fracture frailty affected the outcome of rehabilitation in older persons with proximal hip fracture. The FI-MDS frailty index and the Rockwood Clinical Frailty Scale were used as comprehensive measures of the patients' health status before fracture. The Functional Independence Measure (FIM) on discharge served as a measure of rehabilitation outcome.
The Institutional Review Board approved this retrospective observational study and waived the need for obtaining patients' informed consent. The study was conducted in a 40- bed rehabilitation department that admits mainly orthopedic patients. Included were consecutive patients aged 65 years or older transferred from orthopedic surgery to the geriatric rehabilitation ward. Excluded were non-cooperative subjects, those having an infected operation site, and those temporarily prohibited to tread. The following study parameters were appraised, each-one by independent observers: the FIM at the time of admission, FIM at the time of discharge, the absolute functional gain (calculated as the difference between FIM discharge and FIM admission, i.e. ΔFIM), the daily gain of FIM (calculated by dividing the absolute functional gain by the length of stay in rehabilitation, i.e. ΔFIM/LOS), the Rockwood Clinical Frailty scale (FI Rockwood), the frailty index calculated from the Minimum Data Set document (FI-MDS), the Mini–Mental State Examination of Folstein (MMSE), and the length of stay in rehabilitation (LOS).
Pre-fracture frailty was assessed by physicians who were directly involved in the patients' care. Two frailty tools were used, the FI-Rockwood [22] and FI-MDS, the latter was calculated from the Minimum Data Set document [23]. From the MDS document a list of 58 deficits was derived representing multiple functional domains. Each deficit was assigned either 0 (absence of the condition or attribute) or 1 (presence of the condition or attribute). The body mass index was assigned score 0 unless it was < 18.5 kg/m2 or ≥ 30 kg/m2, in which case a score of 1 was assigned. Medication usage was scored according to the number of medications used: 6-9 score 1; 10-14 score 2; 15-19 score 3; > 20 score 4. The mean of the deficits was expressed as a proportion of the total 58 points, ranging from 0 (no deficits) to 100% (58 deficits) [23]. By the Rockwood Clinical Frailty Scale the examiner’s intuitive perception of a patient’s disability and cognitive impairment was represented by a score ranging from 1 (robust health) to 7 (complete functional dependence) [22]. The Mini–Mental State Examination (MMSE) of Folstein [24] was used assess the patients' cognitive state at the time of admission.
The Functional Independence Measure (FIM) is used in rehabilitation to explore an individual's physical, psychological, and social functions and to monitor the progress under rehabilitation. The FIM has two subscales: the motor subscale, consisting of 13 items related to self-care, transfers, and locomotion, and the cognitive subscale, consisting of 5 items related to comprehension, expression, and memory. Each item is assigned a rating of 1-7, where 1 denotes the necessity for assistance and 7 denotes complete independence [25]. The 'FIM admission' is administered within 3 days of admission to rehabilitation and the 'FIM discharge' within 3 days before discharge by the same team. According to common knowledge, total FIM on discharge ≥90 or motor FIM on discharge >58 signify that a person can be discharged home [6].
Rehabilitation involved the diagnosis of a person’s problems and needs, defining rehabilitation goals, and therapeutic interventions in order to regain maximum self-sufficiency. Rehabilitation was provided by a multidisciplinary team consisting of physicians, occupational therapists, physical therapists, social workers, speech and language therapists, dietitians, and nurses. The patients received 5 days per week standard physical therapy (i.e., walking, climbing stairs, balance, muscle strength, and range of motion) and occupational therapy (i.e., basic ADL, instrumental ADL, and environment advice). The outcome of rehabilitation was evaluated by three measures: 1). the absolute functional gain from admission to discharge, i.e. ΔFIM, 2). FIM discharge ≥ 90, and 3) motor FIM discharge >58.
We assessed which degree of pre-fracture frailty is compatible with rehabilitation success, the latter corresponding to FIM discharge ≥90 or motor FIM discharge >58. Statistical analysis by MedCalc® Statistical Software version 19.8 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2021) used descriptive statistics, Pearson’s correlation, Receiver Operating Characteristic curve, and logistic regression analysis, as appropriate. P < 0.05 was considered significant.
The data of 45 consecutive patients who met the inclusion criteria were reviewed. Five patients could not complete rehabilitation because of intercurrent illness needing hospitalization and were excluded from the analysis. Among the remaining 40 subjects there were 31 women and 9 men, their mean age was 80 years. The FI scores, MMSE, FIM on admission, FIM on discharge, motor FIM on discharge, ΔFIM, LOS and ΔFIM/LOS are shown in Table 1.

The mean ΔFIM (FIM improvement from admission to discharge) was 16.6 points (SD 9.9). The mean functional gain was of 0.8 FIM points per day (SD 0.6). The correlations between pre-fracture frailty by either method and FIM at the time of discharge are shown in Figure 1.
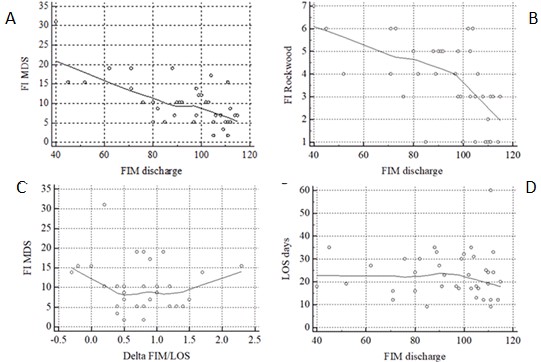
Also represented in this figure are the pace of FIM improvement under rehabilitation (delta FIM / LOS) and the correlation between discharge FIM and LOS. It is noticed that a longer LOS compensated for a slower pace of improvement as to attain greater FIM at the time of discharge.
Alike FI MDS, FI Rockwood correlated poorly with ΔFIM/LOS: R -0.15, p 0.35. Two measures serve as surrogate indicators that a patient is fit to be discharged home: a total FIM discharge ≥90 and a motor FIM discharge >58 (17). In the present cohort, five patients scored FIM ≥90 on admission; their number increased to 20 at the time of discharge.
Logistic regression analysis showed that pre-fracture frailty, by FI MDS as well as by FI Rockwood, is associated with and determines success in rehabilitation (Table 2).

By means of receiver operating characteristic (ROC) curves the performance of pre-fracture frailty scores in achieving determined FIM discharge thresholds were analyzed. The data is shown in Table 3 and Figure 2.

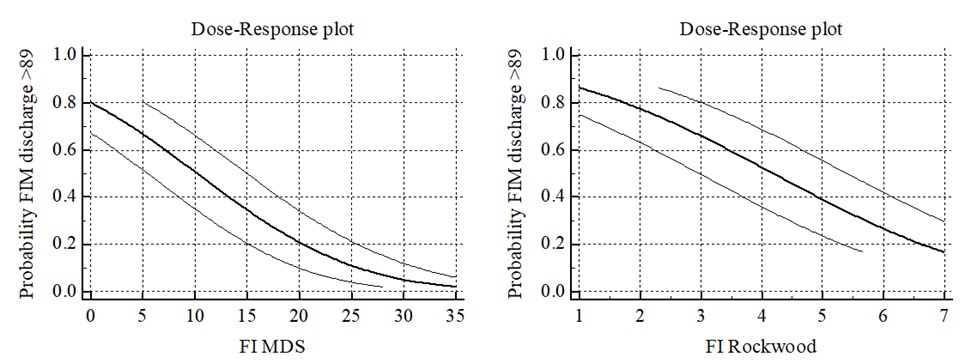
For total FIM discharge ≥90, pre-fracture FI MDS best cutoff was ≤12.1, sensitivity 88.5% and specificity 53.8%; pre-fracture FI Rockwood best cutoff was ≤4, sensitivity 73% and specificity 53.8%. Similar results were observed for motor FIM discharge >58. Dose response plots provide graphical illustration of frailty score-related probability that patients will reach desired total FIM threshold at the time of discharge. Similar constructs were seen for motor FIM discharge >58 (not shown).
An additional analysis, by setting the total FIM discharge threshold at ≥85, showen comparable results as for total FIM discharge threshold ≥90.
The question addressed was whether frailty scoring can be to predict success in rehabilitation after hip fracture. Can severity of frailty predict, better than clinical judgment, situations when rehabilitation after hip fracture is futile? A positive answer to this question would be important for clinical decision making. The short time frame needed to answer this question in rehabilitation after hip fracture offered the prospect to arrive at a clear answer. Indeed, pre-fracture frailty correlated with FIM on discharge, but neither frailty tool was sensitive and specific enough to predict success in rehabilitation and the length of stay in rehabilitation.
The outcome of rehabilitation is difficult to measure because several outcomes are relevant and because the relevant outcomes are affected by multiple factors in addition to treatment [26]. In practice, the use of one representative predictor of outcome, e.g., total FIM discharge or motor FIM discharge, is a necessary compromise. The validity of FIM for determining outcomes of rehabilitation is well established [27]. In a study of 117.168 Medicare beneficiaries receiving inpatient rehabilitation for hip fracture a discharge motor FIM score 58 yielded the best balance in sensitivity and specificity for discriminating patients discharged to the community from those discharged to an institution. FIM motor was equally effective as FIM total and more effective than FIM cognition to this aim, Moreover, FIM motor ratings alone were as effective as a multivariable model in discriminating patients discharged to the community from those discharged to an institution [6]. From a clinical perspective, a diagnostic tool based on a single standard measure and a defined threshold of success (e.g. discharge FIM) is more practical and meaningful than values obtained from a composite model [6], and it also is most popular [28]. Both indices, the total FIM discharge and motor FIM discharge, were used in our study.
Frailty as a predictor of short-term functional recovery after a pathological event has been investigated in diverse conditions, such as trauma, general surgery, chemotherapy, kidney transplantation, and decisions to treat hyperparathyroidism [17,23-28]. A comprehensive literature survey investigated the association of frailty (by means of the Clinical Frailty Scale) with an outcome, mostly in hospitalized patients. Frailty was predictive in 74% of the cases, highlighting its utility in the care of older patients [29]. On the other hand, in the assessment of cardiac preoperative risk, incorporating frailty in existing models require further validation and have not been widely adopted [30,31]. Research is needed to quantify the predictive ability of validated frailty instruments in the context of different surgical procedures and existing surgical risk indices [32,33].
Functional recovery after hip fracture was connected to the degree of frailty in previous [5,6,28] as well as in the present study. The lower was the pre-fracture frailty score the higher was the probability of success in rehabilitation. Both frailty tools, the FI MDS and FI Rockwood, fitted well to the population of the present study, where the patients' physical and cognitive limitations would impede on performance of motor tests and on self-reporting. Pre-fracture FI MDS and FI Rockwood corelated strongly (p <0.0001) with FIM discharge score ≥90 and motor FIM discharge score >58 (Figure 1). However, their predictive accuracy was disappointing: for FIM discharge score ≥90 the best discrimination of success from failure was provided by FI MDS 12.1 with 88.5% sensitivity but merely and 53.8% specificity. Comparable results were found for FI Rockwood. Beyond commonsense used for the first triage, frailty tools performed with insufficient specificity in predicting the outcome of rehabilitation. Moreover, the frailty tools were inaccurate in predicting the pace of improvement under rehabilitation. For the disadvantaged, a longer stay in rehabilitation compensated for slower improvement (Figure 2).
Frailty impacts the outcome of rehabilitation after proximal hip fracture. Yet, frailty tools are not useful to predict success of rehabilitation nor the necessary length of stay in rehabilitation. Translating frailty scores into clinically sensible tools to predict outcomes remains an aim for future studies.
Oxana Zalyesov in the design of the study, acquisition of data; Muhamd Badarny in assessment of patients’ FIM; Natalia Zaygraykin in the planning the study, review of the literature, data analysis; Jochanan E. Naschitz, conceiving and planning, data analysis, writing the manuscript
There were neither personal nor financial conflicts of interest to this study.
No funding was provided for this study.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
